On Tuesday night I got to take call, and I think it was my most fun day/night so far in med school. I got to see a bunch of operations I'd never seen before, and we had some good trauma. The general surgery residents cover call for the trauma service, so I got to see some normal general surgeries, that I should've seen last year on general surgery, like a below-the-knee amputation (BKA), which was SOOOOO cool....The residents here are so nice, and not at all like this guy:

They love to teach and let you help, so a great time was had by all. They were halfway through an APR (abdominal-perineal resection - when the patient has a necrotizing infection in their nether regions, and the flesh down there has basically rotted away, you have to go in and clean it all out, and try to find enough skin to stretch over what's left - a very complicated operation) when I got there, so I watched the end of that, and then after that we did the BKA, which I got to scrub in for, and help file down the end of the bones with what was basically a giant metal nail file. So much fun!
*****
The most serious case of the night was a patient who had a motorcycle accident, and basically not a scratch on him. He basically only had a bit of abdominal/LUQ (left upper quadrant) pain, and was joking with us....When we were cutting off all his clothes and putting a Foley (tube that goes in your urethra to your bladder - not very fun) in, he was like "This isn't at all like the Discovery Channel!!" He was a really nice guy. Unfortunately he turned out to have a Grade 4 (Grade 5 is the worst) splenic laceration. On CT, his spleen looked like hamburger, basically. Here is where your spleen is:
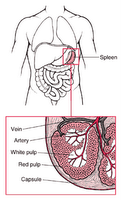
And this is what it looks like when it's on the scrub nurse's table:

The spleen above has a pretty minor laceration. So your spleen is what holds a lot of the cells that help pick the bad stuff (like viruses and bacteria and dead cells) out of your blood. So it has a VERY good blood supply, and holds a lot at any given time. It's also pretty important to have - people that don't have one are very susceptible to overwhelming infections later in life. And what's funny is that most people don't know whether they have one or not. When you ask a patient who has a scar over their spleen area if they had a splenectomy, many of them don't know what you're talking about. Kind of strange that so many people let surgeons dig around in their bellies without much concern over what they have left in there....So the spleen has a lot of blood running into/through it, and the blood carries hemiglobin, which carries oxygen, without which your cells can't live. This is hemiglobin:

In this case, our patient's hemiglobin level before we took him to the OR was 6 (normal for a guy his age/size would be 14-15 or so, and from 5-below, the patient could die very soon - usually from a cardiac arrhythmia, because the heart is starved of oxygen). Intraoperatively, it went down to 4. He was not doing very well. The reason we didn't give him any more blood was that he was a Jehovah's Witness, and they won't accept any blood products. Before we went to the OR we told him how dangerous this was and that there was a good chance he could die, and he was just like, "Can't you use those blood expanders?" No, real life is not like TV. So after we came out of the OR we talked to the family, but they said no. That was what he wanted. So there was basically nothing we could do. The next morning, his hemiglobin was 3. I imagine his blood was probably almost clear, having so few red blood cells left....His vasculature was basically full of normal saline instead of blood. He died that night.
******
Take home lesson: Jehovah's Witnesses probably shouldn't ride Harleys.