So I was standing out at the front of my building today, waiting for my bus, and I was literally grinning from ear-to-ear, just so happy to be here, seeing what I'm seeing every day. The things they see on an every-day basis here, many doctors won't ever see, much less have the opportunity to get to treat. I got to see one really neat, rare thing today, and then I had another really cool thing that we had to rule out in a patient, so we had to do a bunch of investigating because no one knew for sure what to do. The neat thing here, is that everyone here is an expert on something or other. These are the best people in the world you can call with your questions, and they're right in our building!
I can't really tell you guys any specifics, but I thought I'd put some info about some of the oddball things that come through a place like the NIH. So the next time either of these conditions pop up on a "House" episode, you guys can tell your friends, "Oh yeah, methylmalonic acidemia, that's kid stuff!"
******
So the first "zebra" is something called methylmalonic acidemia (MMA). It's an autosomal recessive enzyme defect (meaning that both parents have to carry a recessive, or "hidden" gene that they carry but don't express themselves) that you're born with. It means you're missing the enzyme you need to process fats and proteins. The patients have vomiting, dehydration, hyperglycemia (high blood sugar), hypotonia (weak muscle tone), recurrent infections and lethargy. It's usually found in infancy, and its effects can range from mild to life-threatening. Babies can look fine early on, but when they start eating more protein, then the effects start showing. There are some pictures of children with it on the internet, but I don't think that's really a nice thing to post, because you don't know who posted those pictures, and if they got the patient's consent, etc., so instead I'm showing you this incredibly fascinating flow chart of where the enzyme defect is:
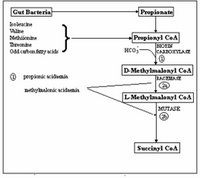
So basically whenever you have an enzyme defect, that means that the process that enzyme was meant to facilitate isn't getting done, and that the precursors for that reaction are piling up somewhere as they're not getting used, and this is never a good thing.
Treatment consists of giving other enzymes, and limiting protein intake. So for example, a patient with this disorder may look overweight and have high blood sugar, and look a lot like a regular type II diabetic, but if you check their protein level, it's almost zero, and they're so protein deficient that they are losing their hair and have skin breakdown. And the sad thing about the really rare diseases like this is that it's usually not diagnosed for a long time, leading to a lot of stress for parents. That's why we spend so much time memorizing "zebras" like this for boards - you might never see something like, this, but if you're ready for it, you can save a family a lot of heartache, not to mention the patient's life.
******
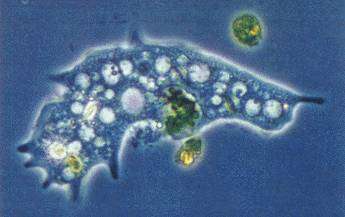
The next cool "zebra" isa bug called called Echinococcus, and I guarantee you, if it hasn't made a "House" or "Gray's Anatomy" episode yet, just give it some time - this bug is pretty darn cool (once again, as long as it isn't in your liver!)!

This is the echinococcus life cycle - it's basically a tapeworm, which can go from a definitive host (often a dog or fox) to an intermediate host (usually a goat, a sheep, or the occasional unfortunate human) and then back out into the environment, eventually to be picked up by another host.

OK, so this is a chest x-ray even I can read. And that's really saying something. In x-rays, air is black, and solid structures are white. So your lungs should be clear (or almost clear) black, and then you can kind of see the sternum and other bones showing up as white. What you shouldn't have is that giant ball in the right lower lobe of the lung (picture the patient facing you)....this is not good. There are three different kinds of echinococcus, and at least one of them really likes people's lungs.
The bug eventually settles wherever it wants to be, and makes a giant cyst that usually isn't found until the patient finds a mass in their abdomen, or starts coughing up blood. Another type of echinococcus really likes livers:

This is a CT: think of this picture as if the patient is lying on a table on their back, with their feet right in front of you. You're looking up through the abdomen. The liver is the big white thing on the right, and what shouldn't be there are all those circles. Big circles in livers are bad. These are giant cysts that echinococcus makes wherever it settles, be it the liver, lungs, or brain (plus some other really random places).
And here's the cool part: you can't just go in and take out the cyst. Why not? one might ask...Because when the cyst fluid with millions of tiny particles of the echinococcus leaks out of the cyst, your body can have an overwhelming allergic reaction and you can die. Not good. So what they do on some of them these days is stick a big needle into the middle of the cyst, aspirate (suck out) the fluid, and then shoot in a drug that kills the echinococcus. Pretty cool stuff. Or you can just give them albendazole and hope it goes away, but that's not very exciting. Who wants that?










































.0.jpg)






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}